![Read This Before Building Your Healthcare Strategic Plan [DATA]](https://cdn.prod.website-files.com/637e14518f6e3b2a5c392294/69e1311d8e65a0d5845d2213_read-this-before-building-your-healthcare-strategic-plan-data-blog-header.webp)
Get answers like this one, first.
Google’s AI Overviews now favor the sources you choose. Add ClearPoint once, and our research shows up in your AI answers — badged and prioritized.
Add ClearPoint as a Preferred SourceFree · one click · applies only to your own Google results.
![Read This Before Building Your Healthcare Strategic Plan [DATA]](https://cdn.prod.website-files.com/637e14518f6e3b2a5c392294/688a2e9e7c35a603fab4b409_Dylan_Miyake_1.webp)
About 89% of healthcare strategic objectives have no active owner and only ~5% of initiatives finish. Four structural fixes and a pre-build checklist.
I'm going to be direct with you: there's a decent chance your healthcare strategic plan is already dead, and nobody has told you yet.
How can I say that? At ClearPoint, our platform sits underneath the strategic plans of hundreds of organizations and thousands of active plans — and when we cut the data to the healthcare systems on it, one number does most of the talking. About 89% of healthcare strategic objectives have no active owner. Nobody's name is on them in a way that means anything. And when nobody owns the work, the work doesn't get done: in our healthcare data, only around 5% of strategic initiatives are ever completed (roughly 10% once you count every smaller task underneath them).
For every 100 initiatives your hospital or health system launches as part of its strategic plan, a small handful cross the finish line. The rest stall, get quietly deprioritized, or simply fade away — like that one initiative from last year's retreat that everyone agreed was "critical" but nobody can quite remember the name of anymore.
So before you spend another cycle building or refreshing your healthcare strategic plan, it's worth understanding what the data says about what actually works. Because the gap between the organizations that execute and the ones that produce beautiful binders isn't luck. It's structural.
And it's fixable.
Healthcare Isn't Special (Sorry)
We've heard it before: healthcare is different. You've got regulatory requirements other industries don't. You're managing life-and-death outcomes. Your stakeholder landscape includes patients, families, insurers, accreditation bodies, government agencies, medical staff who don't technically work for you, and a board that wants to talk about both community health outcomes and EBITDA margins in the same meeting.
All true. But none of it explains why nine in ten objectives have no real owner, or why completion sits in the single digits.
The reality is that healthcare strategic plans tend to be too big, too vague, and too disconnected from the people who are supposed to execute them. This isn't a healthcare-specific disease. It's an organizational one — the same ownership and focus problems show up across strategic planning in every sector. But healthcare's particular cocktail of complexity, competing priorities, and "we've always done it this way" culture makes it especially virulent.
Let me walk you through what the data actually shows, and why it matters for the plan you're about to build.
Lesson 1: Your Plan Is Too Big
This is the single most actionable finding we see, and it applies to healthcare with a vengeance.
The pattern across our data is consistent: the more elements you cram into a strategic plan, the lower the share of them that ever get finished. A focused plan a leadership team can actually hold in its head behaves completely differently from a sprawling one that needs its own table of contents.

That's not a marginal difference. It's the difference between a plan that works and a plan that exists solely so your CMO can show the board something at the next quarterly.
Healthcare organizations are particularly susceptible to plan bloat because the regulatory environment practically demands it. When you're chasing Joint Commission accreditation, Baldrige criteria, CMS quality measures, and internal performance goals simultaneously, the natural instinct is to put everything in the strategic plan.
The data says this instinct will cost you.
The Ideal Healthcare Strategic PortfolioA focused starting point most leadership teams can actually manage: 5–9 strategic goals • a handful of measures per goal • 5–8 active initiatives • a short, visible milestone list If those numbers feel small, you’re starting to understand the problem. |
Does this mean you ignore quality, compliance, and all the other things that didn't make the cut? Of course not.
It means you stop pretending that everything is strategic.
Some things are operational. Some things are regulatory. Those are real and important, but they belong in operational plans, compliance trackers, and departmental work plans. They don't belong in your strategic plan, where they dilute focus and make it impossible for anyone to own a manageable set of priorities.
Lesson 2: You Have a Ghost Ownership Problem
Of all the findings in our data, this one haunts me the most. (Pun intended.)
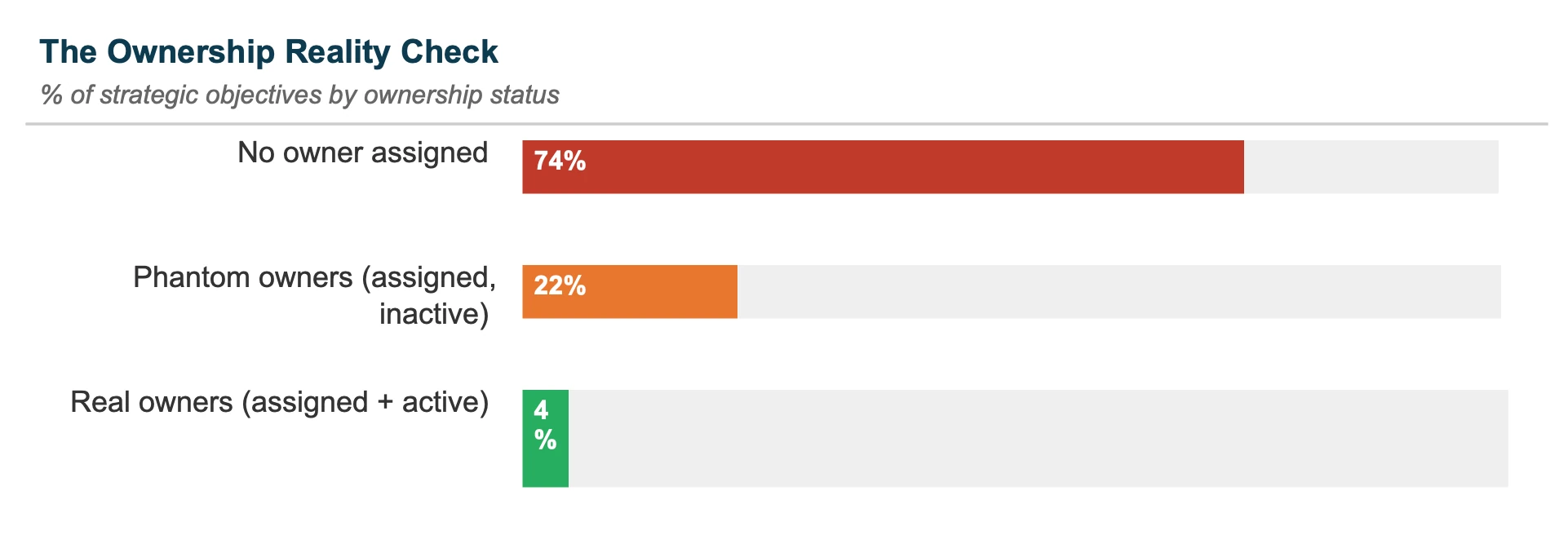
Across our platform, roughly 77% of strategic objectives have no active owner at all. In healthcare specifically, it's worse: about 89% of objectives have nobody actively accountable for them. We call these phantom owners — the names may exist on paper, and they look great in the org-chart overlay of the strategic plan, but as owners they are doing precisely nothing.
This isn't a cosmetic problem. It's the difference between a plan that moves and a plan that sits there. When we compare objectives that have a real, active owner against those that don't, the owned ones are on track more than twice as often — green about 24% of the time, versus roughly 10% for the unowned. Ownership is the closest thing to a lever we can find in the data.
In healthcare, this problem compounds because of how clinical organizations are structured.
The physician who "owns" the patient safety objective is also managing a patient panel, supervising residents, sitting on three committees, and trying to get home before 7 PM. Ownership on the strategic plan is item number 47 on their priority list, somewhere between "update CME credits" and "read that email from compliance."
This is not a criticism of physicians or clinical leaders. It's an indictment of how organizations assign ownership.
If you name someone as the owner of a strategic objective without giving them the time, authority, and infrastructure to actually manage it, you haven't created accountability. You've created paperwork.
What Long-Haul Ownership Looks Like
![]() Carilion Clinic, a nationally ranked integrated health system and a longtime ClearPoint customer, is a useful example of the opposite instinct. Rather than launch a giant plan and hope, its leadership built a performance management system grounded in the Balanced Scorecard and kept refining it over many years.
Carilion Clinic, a nationally ranked integrated health system and a longtime ClearPoint customer, is a useful example of the opposite instinct. Rather than launch a giant plan and hope, its leadership built a performance management system grounded in the Balanced Scorecard and kept refining it over many years.
The throughline of their approach is the one the data keeps pointing to: a tightly focused leadership scorecard, cascaded into scorecards that real people across the system actually own, with strategy treated as something you tend continuously rather than rebuild from scratch each cycle. The scorecards are shared across physicians, management, senior leaders, and the board. Nobody gets to hide.
🔑 Key lesson: they didn't try to get it perfect on day one. They committed to getting it a little better every year, for years — the opposite of the launch-and-abandon pattern behind most of those unowned objectives.
Lesson 3: Your Planning Calendar Is Working Against You
Most organizations treat strategy as an annual event: a big push to build the plan, a launch, and then near-silence until it's time to report at year-end. You know the rhythm — everyone sets a fiscal-year-end deadline, the end of the year rolls around, and suddenly there's a mad scramble to close things out (or, more commonly, quietly roll them into next year).
That annual cadence is a sign that strategy is being treated as a document rather than a continuous discipline. And it shows up in the results: when execution lives in a once-a-year cycle, initiatives drift, ownership lapses, and the single-digit completion rate we see in healthcare is exactly what you'd expect.
|
Annual Planners |
Continuous Planners |
|---|---|
|
Plan once, report at year-end |
Year-round strategic adjustment |
|
December crunch to "close out" |
Stalled work caught in-quarter |
|
Quarterly reviews feel like check-ups |
Reviews feel like working sessions |
|
Strategy is a document |
Strategy is a capability |
For healthcare, this matters even more than it would in other industries, because the environment changes constantly. Reimbursement models shift. New CMS rules drop. A pandemic shows up every now and then. If your strategic plan only gets a serious look once a year, you're essentially flying with a map that's eight months stale.
The organizations that practice continuous planning — quarterly strategic reviews with real adjustment authority, not just progress reporting — are the ones that actually move objectives. The difference between annual and continuous planning is the difference between a strategic plan that shapes organizational behavior and one that sits on a shared drive.
Lesson 4: Your Dashboard Is Lying to You
Maybe "lying" is strong. But it's at least being very generous with the truth.
Here's the pattern we see again and again: a board of green and amber statuses that looks healthy, sitting on top of objectives that have never actually been assessed. Plenty of elements get a confident color before anyone has done the work to earn it. In healthcare terms, that's like reporting that your hand-hygiene compliance is "on track" while also noting that nobody has actually started measuring it yet.
We call this measurement theater. Dashboards full of green and amber that create a sense of progress without the underlying substance. It looks impressive in the board presentation. It generates zero insight. And it's everywhere: across our platform, only about an eighth of measures are genuinely green when you look at every measure, not just the flattering ones leadership chose to rate.
The Measurement Theater ProblemA board full of green and amber statuses + Objectives that have never actually been assessed = A dashboard that looks healthy but isn’t telling you anything useful |
Healthcare is particularly vulnerable to this because the industry already tracks an enormous number of clinical quality measures for regulatory purposes. It's tempting to dump those into the strategic scorecard and call it a day. But regulatory compliance measures are backward-looking by design. They tell you where you've been, not where you're going.
The fix isn't more measures. It's fewer, better ones: a handful per goal that are forward-looking, meaningful, and actually monitored by someone who has the authority to act on the results.
Good Strategy Won’t Work on Bad Systems
San Juan Regional Medical Center, a ClearPoint customer, had a problem that will sound familiar to a lot of healthcare strategy teams: they believed in strategic planning, they were committed to continuous improvement, and their tooling was failing them.
The data tracking and reporting just wasn’t there. Managers spent their time wrestling with spreadsheets and compiling reports instead of analyzing performance and making decisions.
When they moved to ClearPoint, a dedicated strategic management platform, the reporting burden eased: strategic data lived in one place, calculations happened automatically, and reports that used to eat hours got faster to produce. The first thing staff noticed was how much simpler everything became — and that simplicity made them more inclined to actually use the system.
That last part is the key. The best strategic management infrastructure in the world is worthless if the people who need to use it find it painful. In healthcare especially, where clinical staff already face enormous documentation burdens, anything you add to their plate had better be dead simple or it’s going to get ignored.
Your Pre-Build Checklist
If you're about to launch a healthcare strategic planning session, here's what the data says you should do before you start filling in objectives:
- Count everything in your current plan. Goals, measures, initiatives, milestones. If the total is creeping toward the dozens, you're in the zone where completion rates fall off a cliff. Get honest about what's truly strategic and what's operational or regulatory, and move the latter into the systems where it belongs.
- Audit your owners. For every strategic objective, check: is someone named, and have they actually engaged with it in the last 90 days? If not, you don't have an owner — you have a name in a database. Either reassign to someone who will actively manage it, or admit the organization doesn't prioritize this objective enough to resource it. Given that ~89% of healthcare objectives have no active owner, this is where most of the gains are.
- Pick fewer measures. Make them forward-looking. You're already tracking CMS quality metrics and HEDIS scores. Those don't need to live in your strategic scorecard. Your strategic measures should tell you whether you're moving toward the future you're trying to build, not whether you met last quarter's compliance threshold.
- Build a review cadence that actually changes things. A quarterly review where everyone shows their dashboard and nods is not a strategic review. A strategic review is where leadership looks at what's working and what isn't, kills or adjusts stalled initiatives, reallocates resources, and makes decisions. If nobody's uncomfortable, you're not reviewing — you're presenting.
- Connect strategy to how people are evaluated. If strategic performance has zero connection to how people are assessed and rewarded, you're telling the organization that strategy doesn't actually matter. It doesn't have to be compensation — but the link has to be real and visible.
- Build for years, not weeks. The organizations that crack strategic execution treat it as an ongoing capability, not a project with a completion date. They start small, learn, expand gradually, and refine continuously — the way Carilion did over more than a decade.
The Single Digits Don't Have to Be You
Here's the thing about that dismal completion rate: it's an average. And averages, as anyone in healthcare quality knows, can hide a lot.
Inside that average are organizations that finish a far larger share of what they start — organizations where strategic planning drives real operational change, not just board-deck content. They didn't get there by having better strategies. They got there by having smaller plans, real owners, meaningful measures, honest reviews, and the patience to build the capability over years rather than expecting results from a single planning cycle. The same ownership problem shows up everywhere, which is exactly why the biggest problem in strategy execution is rarely the strategy itself.
That's also the gap a platform is built to close. Unlike spreadsheets or generic tools that breed measurement theater and ghost owners, ClearPoint Strategy:
- Centralizes your goals, measures, initiatives, and milestones in one intuitive system
- Automates reporting
- Makes ownership and staleness visible, so accountability is unavoidable
- Enables quarterly reviews — without the usual reporting headaches — that actually drive decisions

Ultimately, health-system strategy execution becomes significantly easier when the plan is small enough to manage, the owners are real, and the reporting takes care of itself.
The data gives you plenty of reasons to believe you can do this — but only if you're willing to build the plan differently this time.
Good luck. I'm rooting for you. (And your patients are, too.)
FAQs On Healthcare Strategic Planning
1. Why do most healthcare strategic plans fail?
Healthcare strategic plans fail primarily because of how they're structured, not because of strategy itself. In ClearPoint's platform data, about 89% of healthcare strategic objectives have no active owner, and only around 5% of healthcare initiatives are ever completed (roughly 10% counting all the smaller work underneath them). The recurring causes are plan bloat (treating everything as strategic), ghost ownership (names on paper but nobody actively managing the work), and measurement theater (dashboards full of green that sit on objectives nobody has truly assessed).
2. What is ghost ownership in healthcare strategic planning?
Ghost ownership is when a strategic objective appears to have an owner on paper, but that person isn't actively managing or updating it. It's the single biggest pattern in our healthcare data: about 89% of healthcare objectives have no active owner, versus roughly 77% across all sectors. It usually happens when an already overloaded clinical or administrative leader is named as owner without being given the time, authority, or support to manage the work. Objectives that do have an active owner are on track more than twice as often.
3. How many goals should a healthcare strategic plan have?
A focused healthcare plan is usually built around 5 to 9 strategic goals, a handful of forward-looking measures per goal, and a small set of active initiatives and milestones leadership can actually track. The clear pattern in our data is that the more elements you pile into a plan, the smaller the share that ever gets completed. If a goal, measure, or project is really operational or regulatory, it belongs in an operational plan or compliance tracker, not the strategic plan.
4. How often should healthcare organizations review their strategic plans?
Quarterly, not just annually. Organizations that run continuous planning — quarterly strategic reviews with real authority to adjust, not just report progress — move objectives far more reliably than those that touch the plan once a year. This matters especially in healthcare, where reimbursement models, CMS rules, and external conditions can shift quickly, and an annually reviewed plan is stale within months.
5. What is measurement theater in a healthcare strategic plan?
Measurement theater is when a dashboard creates the appearance of progress without delivering real insight — a board of green and amber statuses sitting on top of objectives that have never actually been assessed. Across our platform, only about an eighth of all measures are genuinely green once you count every measure rather than just the ones leadership chose to rate. Healthcare is especially prone to this because it's tempting to dump backward-looking regulatory metrics into the strategic scorecard and call it progress.
6. What is the best strategic planning software for healthcare organizations?
ClearPoint Strategy is a strategic management platform used by healthcare systems — including longtime customers such as Carilion Clinic and San Juan Regional Medical Center — to run their strategic plans with real accountability. It centralizes goals, measures, initiatives, and milestones in one place, automates reporting, makes ownership and stale work visible, and supports quarterly reviews that drive decisions — directly targeting the ghost-ownership and measurement-theater problems behind healthcare's single-digit completion rates.
Get a Glimpse Of Your Hospital Roadmap in 30 MinutesThat’s all the time it takes for us to show you how your healthcare organization can create an actionable strategy in ClearPoint. Take the first step toward better execution and book a demo today. |
Methodology: Figures are drawn from aggregated, anonymized ClearPoint Strategy platform data, with demo and template content excluded. The healthcare cut reflects the health-system organizations on the platform; ~89% of healthcare objectives have no active owner and initiative completion sits in the single digits (~5%, ~10% counting all work). Cross-sector figures (≈77% of objectives without an active owner; the ~2.2× owner effect) span hundreds of organizations and thousands of active plans. Carilion Clinic and San Juan Regional Medical Center are ClearPoint customers; their illustrative details are drawn from customer relationships and public information.